

Clinical benign prostatic hyperplasia (BPH) is one of the most common diseases in aging men which can lead to lower urinary tract symptoms (LUTS). The relation between clinical BPH and LUTS is complex, because not all men with clinical BPH develop LUTS and not all men with LUTS have clinical BPH.
As age increases, the prostate gland enlarges, leading to a rising incidence of BPH. Approximately 45% of men over 45 years of age develop BPH, with the prevalence increasing to about 80% in men over 70. According to the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019, there were 94 million cases of BPH worldwide in 2019.
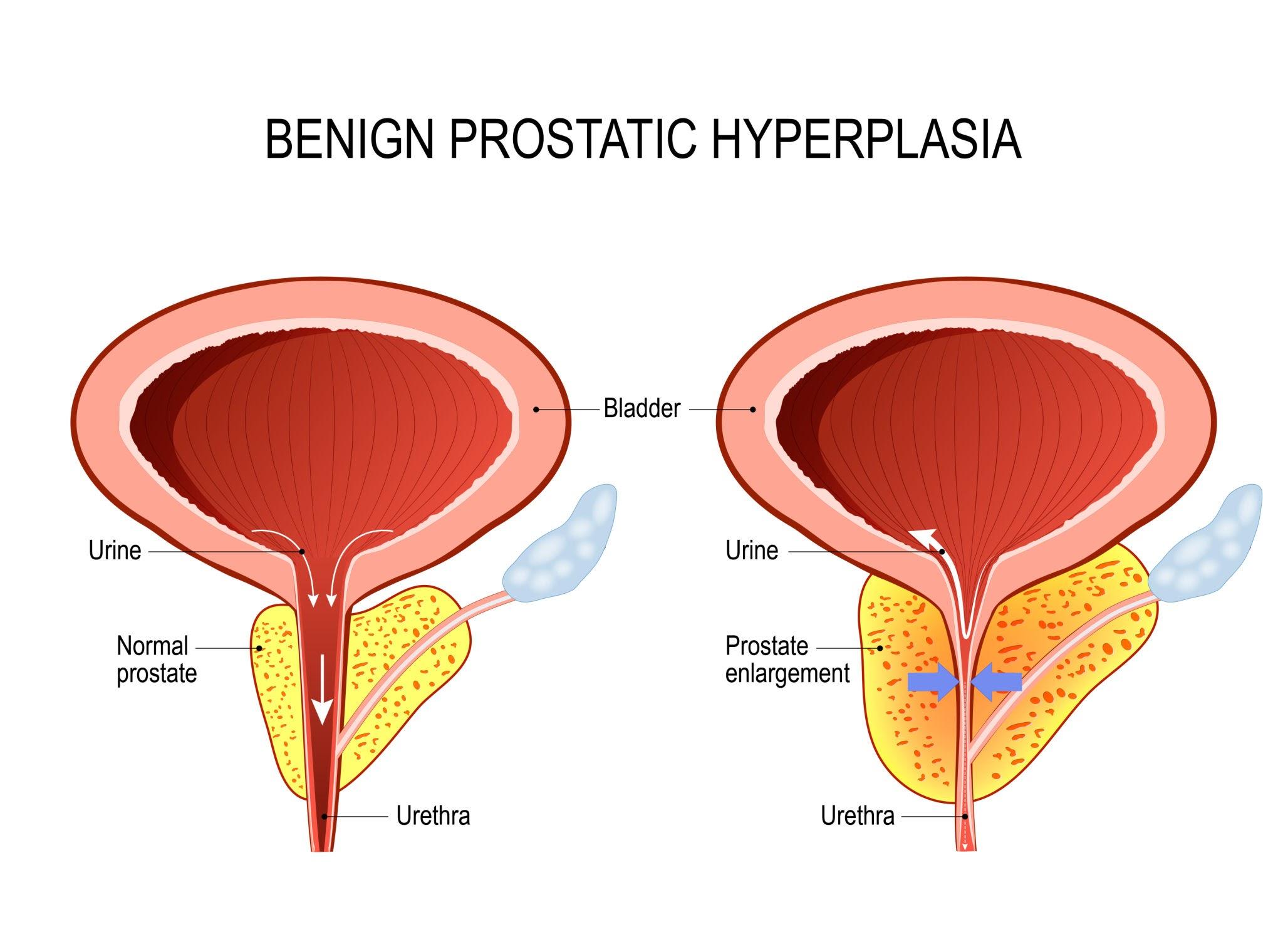
Although BPH is a non-malignant condition, many elderly men suffer from its negative impact on quality of life. The clinical features of BPH involve the progressive development of lower urinary tract symptoms (LUTS) caused by the continuous proliferation of stromal and epithelial cells in the transition zone surrounding the urethra. These symptoms, which include nocturia, difficulty in urination, hesitancy, and frequency, significantly reduce patients’ quality of life, impair mental health, and increase healthcare costs. Furthermore, BPH can lead to adverse events such as urinary tract infections, acute urinary retention, vesical calculi, and acute renal failure. With the aging population, the rising incidence and symptoms of BPH with age contribute to a significant increase in societal burden.
1. Age
The prevalence of BPH rises markedly with increased age. Observational studies from Europe, US, and Asia have also demonstrated older age to be a risk factor for clinical BPH onset and progression.
2. Genetics
Evidence suggests a strong genetic component to BPH. A case-control analysis, in which men below 64 years underwent surgery for BPH, noted that male relatives and brothers had 4-fold and 6-fold increases, respectively, of age-specific risks for BPH surgery. These investigators further estimated that 50% of men below 60 years undergoing surgery for BPH had a heritable form of disease.
3. Lifestyle
It has increasingly been observed that modifiable lifestyle factors substantially influence the natural history of BPH.
a. Diet
There are some indications that both macronutrients and micronutrients may affect the risk of BPH. For macronutrients, increased total energy intake, energy-adjusted total protein intake, red meat, fat, milk and dairy products, cereals, bread, poultry and starch all potentially increase the risks of clinical BPH and BPH surgery, while vegetables, fruits, polyunsaturated fatty acids, linoleic acid, and vitamin D potentially decrease the risk of BPH. With respect to micronutrients, higher circulating concentrations of vitamin E, lycopene, selenium, zinc and carotene have been inversely associated with BPH.
b. Physical activity
Increased physical activity and exercise have been consistently linked to decreased risks of BPH surgery, clinical BPH, histological BPH and LUTS.
4. Metabolic Syndrome
a. Obesity
Studies have consistently found that increased adiposity is positively associated with prostate volume; the greater the adiposity, the greater the prostate volume. Body weight, body mass index (BMI), and waist circumference have all been positively associated with prostate volume in multiple different study populations. Epidemiological evidence also demonstrates that obesity increases the risks of BPH surgery, urinary symptoms progression, and initiation of BPH medical therapy.
b. Diabetes
Physician-diagnosed diabetes, increased serum insulin, and elevated fasting plasma glucose have been associated with increased prostate size and increased risk of prostate enlargement, clinical BPH, and BPH surgery.
c. Lipids
There are relatively few data on potential associations between lipids and BPH. Some studies have shown positive associations while others did not find any association between them.
5. Inflammation
It is likely that inflammation plays a role in the development and progression of BPH, as evidenced by the strong link between BPH and histological inflammation in specimens obtained from prostate biopsies and BPH surgery. Furthermore, inflammatory cytokines are overexpressed in BPH tissues. The underlying causes of prostatic inflammation remain unclear, although there are several hypotheses: 1) response to tissue damage because of infection, 2) autoimmune response, 3) obesity and abdominal fat, because of excess production of inflammatory cytokines from adipose tissue.
Inflammation has been implicated as a primary stimulus for prostate carcinogenesis, and it is possible that BPH represents a non-malignant pathway of unregulated prostate growth promoted by oxidative stress, inflammatory mediators, and insulin growth factors.
BPH arises due to the loss of homeostasis between prostatic cellular proliferation and apoptosis or cell death. This imbalance favors cellular proliferation without intervention. The result is increased numbers of prostatic periurethral epithelial and stromal cells, which can be seen histopathologically. The etiology of BPH is influenced by a wide variety of risk factors, in addition to the direct hormonal effects of testosterone on prostate tissue.
Testicular androgens are required to develop BPH, as dihydrotestosterone (DHT) promotes tissue growth and cellular proliferation by interacting directly with prostatic epithelium and stroma. Testosterone is converted to DHT by 5-alpha-reductase 2 in prostatic stromal cells and accounts for 90% of total intraprostatic androgens. DHT directly influences prostatic stromal and adjacent cells, which affect cellular proliferation and apoptosis.
Common symptoms of BPH include:
a. Frequent or urgent need to pee, also called urination
b. Peeing more often at night
c. Trouble starting to pee
d. Weak urine stream, or a stream that stops and starts
e. Dribbling at the end of urination
f. Not being able to fully empty the bladder
Less common symptoms include:
a. Urinary tract infection
b. Not being able to pee
c. Blood in the urine.
The symptoms of BPH tend to slowly get worse. But sometimes they stay the same or even improve over time. The size of the prostate doesn’t always determine how serious the symptoms are. Some people with slightly enlarged prostates can have major symptoms. Others who have very enlarged prostates can have minor problems. And some people with enlarged prostates don’t have any symptoms at all.
The best ways to reduce the development of BPH are to make lifestyle changes that improve prostate and heart health and take supplements. Exercising at least 30 minutes each day may help prevent BPH or slow prostate growth. Maintaining normal cholesterol, blood pressure, and blood sugar levels is also important. Taking supplements that contain Saw palmetto extract, Tomato powder, and zinc can also be an option.
There isn’t a cure for BPH. However, treatment options are available to help alleviate symptoms. If the patient has mild symptoms, you may not require any treatment. The healthcare provider may recommend regular appointments to ensure BPH doesn’t worsen.
Medication or surgery options include:
a. Medications that relax the muscle in the prostate, which reduces tension on the urethra. Examples include: Tamsulosin, Terazosin, Doxazosin, Alfuzosin, Silodosin.
b. Medications decrease production of the hormone DHT, which can slow the growth of the prostate gland. These medications are most beneficial to people with larger prostates. Examples include: Finasteride, Dutasteride, and herbal ingredients like Saw palmetto extract.
c. Medications that help improve urine flow, like Tamsulosin.
d. Surgery
Several different types of surgery can remove prostate tissue that blocks the urethra. These include:
d.1. Transurethral resection of the prostate (TURP). The urologist inserts a special instrument (resectoscope) through the urethra that allows them to see and remove prostate issue
d.2. Transurethral incision of the prostate (TUIP). The urologist makes two small incisions in the prostate and where the urethra and bladder join (bladder neck) to widen the urethra and improve urine flow
d.3. Transurethral electrovaporization. The urologist uses an electrode to heat the prostate tissue. This turns the tissue cells in the enlarged areas of the prostate into steam.
d.4. GreenLight™ laser treatment. The urologist uses a special laser to evaporate the enlarged prostate tissue. Other names for GreenLight laser treatment include photoselective vaporization of the prostate (PVP) and prostate photovaporization.
d.5. Aquablation®. The urologist uses precise, high-pressure jets of water to remove prostate tissue.
Saw palmetto extract (SPE) is the most commonly used supplement for the treatment of lower urinary tract symptoms (LUTS). Fruit extracts are composed of 90% saturated and unsaturated fatty acids, as well as higher alcohols and sterols. Because of its pharmacological effects such as 5α-reductase inhibition, antiandrogenic action, and α1 receptor and muscarinic receptor binding activity, it has been used as a drug or supplement to improve dysuria caused by BPH.
Tomato extract, the whole fruit of tomato providing the most comprehensive complex of prostate-health-preserving micronutrients, has been shown to be superior to its single-nutrient counterparts in decreasing the incidence of age-related prostate diseases. Supplements in the form of tomato extract are superior to single lycopene supplements because tomato extract contains a complex of components such as lycopene, tocopherol, quercetin, and others. These components work synergistically to help maintain prostate health.
Zinc has been identified as a dietary factor that may play a protective role in prostate cancer. Zinc levels are tightly controlled because it is involved in many physiological processes. Zinc accumulates in the prostate at ten times the level in any other tissue, and this accumulation plays a vital role in maintaining the overall health of the prostate gland.
PT Simex Pharmaceutical Indonesia, as one of the pharmaceutical companies in Indonesia, presents SIMPROSTAT® products as supplements that contain Saw Palmetto Extract 160 mg, Tomato Extract 30 mg, and Zinc Picolinate 12,5 mg. The combination of three herbal components that can help improve benign prostatic hyperplasia.
Reference
.jpg)







